
Introduction
India accounts for approximately 11% of global road crash fatalities while comprising roughly 1% of the world’s registered vehicles, a disproportion that reflects compounded failures across governance, infrastructure, enforcement, and public awareness.1 Delhi, being the national capital and one of the busiest and most crowded cities in Asia, shows this problem very clearly. People who are most exposed on the roads, such as pedestrians, two-wheeler riders, and those working in the informal sector, are the ones who suffer the most. This pattern has also been consistently highlighted in epidemiological studies.2
To address this issue, the Government of India introduced the Motor Vehicles (Amendment) Act, 2019. This law brought in much stricter penalties for traffic violations, offered legal protection to Good Samaritans who help accident victims, and ensured cashless treatment during the ‘Golden Hour’, that is, the first hour after an accident when timely medical care can make the biggest difference in saving lives. While these steps clearly show stronger intent from the government, an important question still remains: have these changes actually made a real difference on the ground?
No legislative framework, no matter how well designed, can operate independently of its social context. Its effectiveness is mediated by the degree to which citizens understand and interpret it, how well they internalise it, and act upon its provisions. This is exactly where health literacy becomes essential. In simple terms, health literacy means having the ability to find, understand, and use health information to make the right decisions.3 This idea applies just as much to road safety. For example, a person who understands how wearing a helmet protects the brain during an accident is far more likely to wear one willingly, compared to someone who sees it only as a rule they have to follow.4
This study was designed to examine where Delhi’s road users stand at this nexus. It explores how people understand road safety, how they perceive the risks of road traffic injuries (RTIs), how aware they are of the health consequences of accidents, and how much trust they place in current policies. Based on survey responses from 100 individuals across the five zones of Delhi, the findings highlight the gaps between what people know and how they actually behave. More importantly, they point to the areas where focused interventions can make the greatest impact in closing these gaps.
Literature Review
The global literature that currently exists on road safety consistently identifies enforcement consistency and public awareness as the two most powerful behavioural determinants of compliance. Naci et al. (2009) demonstrated that countries that consistently enforce seatbelt and helmet rules tend to have much lower death rates, no matter how strict the laws look on paper. What really makes people follow the rules is the feeling that they will actually get caught and penalised, not just how harsh the punishment sounds. This idea helps explain why the higher fines under the Motor Vehicles Act have had mixed results: stricter penalties alone do not work unless people believe they will truly be enforced.5
In the Indian context, Mohan et al. (2009) established that Delhi’s RTI profile is characterised by acute vulnerability among pedestrians and two-wheeler riders, who collectively account for the majority of the serious injuries and fatalities due to road traffic accidents. Delhi’s main roads are built mostly to keep cars moving fast, but in doing so they end up putting others at a disadvantage. There are hardly any separate lanes for cyclists or pedestrians, safe crossing points are often missing, and road signs are not always clear or consistent. Because of these design issues, simply enforcing traffic rules is not enough to fix the problem.6
The amended Motor Vehicles Act, 2019 has attracted cautious academic assessment since its enactment. Tiwari (2020) pointed out that simply increasing penalties is not enough on its own; there also needs to be strong enforcement and better detection systems in place to make those penalties truly effective over time.7 Similarly, Dandona et al. (2020) found that while people initially followed the rules more closely after the Act was introduced, this improvement did not last. As enforcement became less consistent, compliance began to drop again. This reflects a common trend: when policing is highly visible, people tend to follow rules more strictly, but that effect fades quickly once the intensity of enforcement decreases.8
Delhi’s domestic legislative trajectory under the Motor Vehicles Act sits within a broader global policy architecture that has hardened considerably since 2020. In August 2020, the UN General Assembly adopted Resolution A/RES/74/299, proclaiming the second Decade of Action for Road Safety 2021–2030 and setting an explicit target of preventing at least 50% of road traffic deaths and injuries over that period.9 The accompanying Global Plan, released by the WHO and the UN regional commissions in October 2021, frames this target through a Safe System approach that treats human error as inevitable and calls for infrastructure, vehicles, speeds, and post-crash care to be designed around that reality rather than around perfect compliance.10 Read against this global benchmark, the Motor Vehicles (Amendment) Act, 2019 functions as India’s principal domestic instrument for pursuing the Decade of Action’s targets, but the Act predates the Global Plan by two years and was conceived primarily as a penalty-and-deterrence reform rather than as a Safe System framework. The persistent gap this study investigates, between legislative intent and everyday road-user behaviour, is therefore not only a matter of domestic enforcement capacity but also a live question of whether India’s road safety policy architecture is converging with or diverging from the systems-level orientation that the Decade of Action prescribes for its 2030 target.
More recent Indian scholarship has continued to document the gap between legislative reform and behavioural change in the years following the pandemic. A 2024 systematic review of Indian road safety research found that the bulk of empirical work on safer road users has concentrated on education, knowledge, and perception of risk, and concluded that most crash victims continue to come from lower socioeconomic backgrounds, framing road safety in India as inseparable from questions of social equity.11 Qualitative work has begun to surface the lived dimension of this gap. A 2024 qualitative study of traffic police personnel in Manipal examined enforcement officers’ own perceptions of young riders’ road safety behaviour, underscoring that the people tasked with translating legislative penalties into everyday compliance often experience the same disconnect between rule and routine practice that this study finds among ordinary road users.12 Separately, a 2024 qualitative study of college students in Madurai who had survived road traffic injuries documented that the consequences of RTIs extend well beyond physical recovery into sustained psychological and social disruption, a dimension that Indian road safety messaging has historically under-addressed and one that this study’s findings on health literacy directly engage.13 Taken together, this body of post-pandemic literature reinforces the view that closing India’s road safety gap requires attention not only to enforcement design but to the equity, psychological, and communicative dimensions that purely punitive frameworks tend to overlook.
Looking at road safety through the lens of health literacy is still relatively new in South Asia. Studies such as that of Brijs et al., conducted in Europe, show that people who better understand the physical and psychological consequences of road accidents are more likely to follow safety practices regardless of whether police enforcement is visible.14 This distinction matters precisely because it locates the determinant of safe behaviour in internalised understanding rather than in the probability of detection, which is the structural condition the Decade of Action’s Safe System approach also relies upon: a road user who understands why a measure protects them is less dependent on continuous, visible enforcement to comply with it.
Don Nutbeam’s framework offers the most structurally precise account of how this internalisation operates, and it is the model this study uses to interpret its own health literacy findings in the results section.15 He describes health literacy as operating across three progressively deeper levels:
• Functional literacy: simply knowing that a rule exists (for example, that wearing a helmet is required).
• Communicative literacy: understanding why the rule matters for one’s own safety and the well-being of others.
• Critical literacy: being able to apply this understanding in real-life, complex situations on the road.
In the Indian context, most road safety campaigns tend to stop at the first level, telling people what the rules are, without helping them truly understand or internalise why those rules matter or how to apply them in everyday traffic situations.
An equally critical dimension is equity. Populations with low literacy rates, people working in the informal sector, and peripheral urban residents face a dual disadvantage: they are both more exposed to RTI risk and less effectively reached by existing awareness mechanisms.16 Addressing this structural exclusion is not just a minor policy concern; it is essential if Delhi is serious about bringing down its RTI burden in any meaningful way.
Methodology
A. Study Design
This study used a cross-sectional survey design, which is well suited to understanding people’s perceptions, knowledge, and attitudes at a specific point in time. Data were collected in February and March 2026 using a structured, self-administered questionnaire that was shared with participants through Google Forms.
B. Sampling and Participants
A purposive-cum-convenience sampling approach was adopted to recruit 100 road users across all five administrative zones of Delhi: North, South, East, West, and Central Delhi. The convenience component governed the primary mode of access, as participants were reached through a self-administered, digitally distributed questionnaire, which by design favoured respondents with smartphone access, digital literacy, and discretionary time to complete an online form. The purposive component was layered onto this access pathway to deliberately counteract its narrowing effect: outreach was directed, as far as the sampling frame allowed, toward achieving representation across all five administrative zones rather than concentrating responses in any single part of the city, and toward securing variation in occupation (students, private-sector employees, self-employed individuals, government employees, professional drivers, and healthcare workers), age bracket, and primary transport modality (private vehicle, two-wheeler, public transport, and pedestrian travel). This purposive targeting was applied as a directional sampling effort rather than as a fixed quota system; no minimum thresholds were set for individual zones, age brackets, or occupational categories, and the achieved distribution reported in the results section reflects the outcome of this effort rather than a pre-specified stratification design. Taking part in the survey was completely voluntary. Before responding, participants were given a clear consent statement explaining that their answers would remain anonymous, would be used only for academic purposes, and that there were no right or wrong answers. No personally identifying information was collected.
C. Instrument
The questionnaire comprised 25 structured items across six thematic sections: (A) Demographic and Socio-contextual Profile; (B) Road Safety Awareness and Knowledge; (C) Perception of RTI Risk Factors and Vulnerable Groups; (D) Health Literacy and Personal Road Safety Behaviour; (E) Policy Effectiveness, Community Engagement, and Social Determinants; and (F) Open-Ended Responses. The questionnaire used a mix of question types (single-choice, multiple-choice, five-point rating scales, and ranking questions) in an effort to capture different kinds of responses. Two ranking items were embedded within this structure to capture relative rather than purely categorical judgements: Q13, situated within Section C, asked respondents to rank five commonly cited contributory factors for road traffic injuries (speeding and reckless driving, poor road infrastructure, distracted driving, weak enforcement, and drunk driving) in order of perceived importance, while Q23, situated within Section E, asked respondents to rank or rate policy and socioeconomic determinants of road safety compliance, including enforcement visibility, awareness-campaign reach, and socioeconomic status. These ranking items were included specifically to allow the relative weighting of competing factors to be assessed using mean rank scores, which descriptive frequency counts alone could not capture, and their results are reported in the perception and policy-effectiveness sections respectively. The instrument also included two open-ended questions, allowing participants to share their thoughts in their own words and helping to add depth and context to the findings.
D. Data Analysis
Quantitative data were analysed using descriptive statistics, mainly through frequency distributions and percentage calculations. For ranking-based questions (Q13 and Q23), mean rank scores were used to determine the relative importance of different options. In the case of multi-select questions, responses were analysed by calculating how often each option was chosen as a proportion of the total number of respondents.
For the qualitative component, open-ended responses (n=46 for Q25 and n=19 for the additional comments section) were examined using thematic content analysis. Recurring themes were identified and used to provide context and support for the patterns observed in the quantitative findings.
Results and Discussion
A. Demographic Profile of Respondents
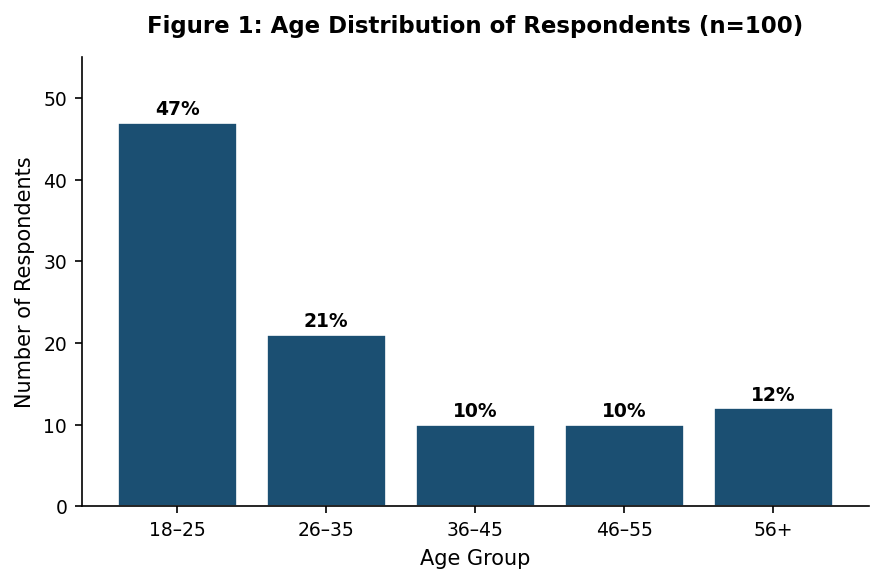
The sample was dominated by younger adults, with 47% falling within the 18–25 age bracket and 21% in the 26–35 range (Figure 1). This age pattern likely reflects who was easier to reach through digital surveys in urban India, as well as a broader reality: young adults make up a large share of people actively using roads in cities. The gender distribution was fairly balanced, with 53% male, 44% female, and 2% identifying as non-binary or choosing not to disclose. This closely mirrors the diverse mix of people who use Delhi’s roads in everyday life.
Figure
Figure 1: Age Distribution of Respondents (n=100)
In terms of occupation, 47% were students, 21% were employed in the private sector, 15% self-employed or in other categories, and 9% in government or public sector roles, with smaller proportions representing professional drivers and healthcare workers. Most participants in the study were well educated: about 39% had undergraduate degrees and another 37% had postgraduate or higher qualifications, while only 1% had education below the secondary level. This strong educational profile actually adds credibility to the findings, because if knowledge gaps are seen even among educated individuals, the situation in the general population is likely to be more pronounced. However, it also limits how far we can apply these results, as the study does not adequately represent people with lower levels of education.
Responses in terms of transport modality reflect the following: 40% used private cars as their primary mode, 26% two-wheelers, 29% public buses or the metro, and 4% primarily walked. This distribution aptly mirrors Delhi’s mixed-mode traffic environment.
B. Road Safety Awareness and Knowledge
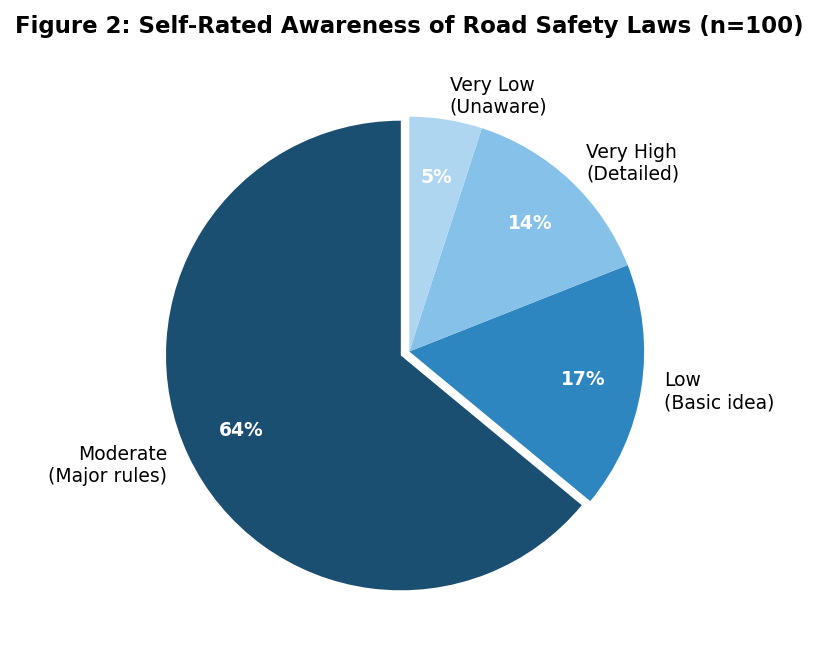
A number of respondents, about 64%, assessed their overall awareness of traffic laws as moderate, indicating familiarity with major rules but not with detailed provisions (Figure 2). In simple terms, they know the basic rules of the road but are not very familiar with the finer details. Only 14% believed they had a high level of awareness, while nearly one in five (22%) admitted their knowledge was low or very low. This pattern suggests a population that has absorbed surface-level road safety norms without developing the depth of understanding necessary to apply them confidently or advocate for them socially, a profile consistent with Nutbeam’s (2008) characterisation of functional health literacy without the communicative or critical dimensions.17
Figure
Figure 2: Self-Rated Awareness of Road Safety Laws (n=100)
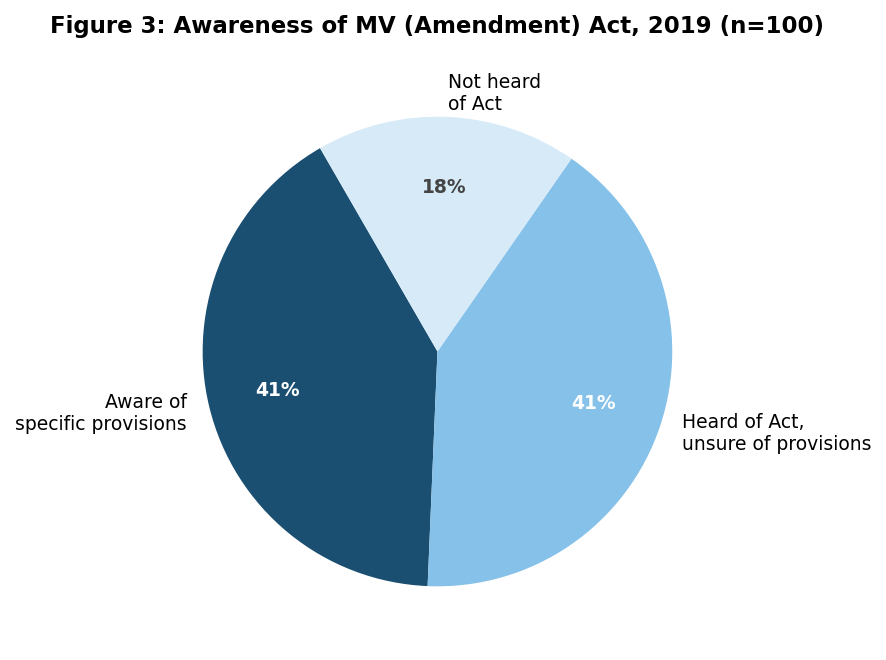
An even split was observed in response to the MV Amendment Act, 2019: 41% reported full awareness of specific provisions, 41% had heard of the Act but were uncertain of its content, and 18% had never encountered it (Figure 3). Even within a mostly educated and urban group, nearly one in five people have never even heard of the Act. This is striking, as this law has been in place for over six years now, and points effectively to the fact that such policies are not being communicated homogeneously to the public at the ground level.
Figure
Figure 3: Awareness of the MV (Amendment) Act, 2019 (n=100)
When people were asked about the specific provisions of the Act, most of them were familiar with the stricter penalties (80%), while fewer people recognised other important features, such as the Good Samaritan Law (43%), mandatory motor insurance (41%), and cashless treatment during the Golden Hour (34%). Notably, 10% of respondents could not identify any provision at all.
What stands out is the relatively low awareness of the Good Samaritan and Golden Hour provisions. This is important because these measures are meant to encourage bystanders to step in during emergencies. If people are not aware of them, they are far less likely to act, which limits the real-world impact of these potentially life-saving provisions, and evidently has not translated from policy into practice at all.
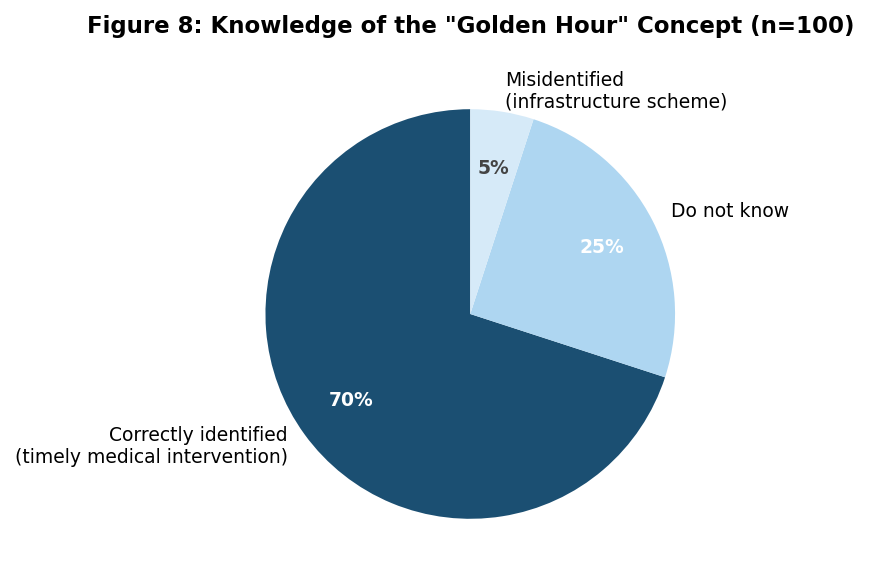
The responses to the Golden Hour question (Figure 8) display a clear pattern: while most participants (70%) correctly understood it as the crucial first hour for life-saving medical care, a significant portion did not, with 25% saying they did not know and 5% even confusing it with an infrastructure scheme. The aspect that stands out again is that even in an educated urban group, one in four people were unaware of this critical concept. This gap reflects a real issue in health literacy and could have serious implications for survival in road traffic injuries.
Figure
Figure 8: Knowledge of the ‘Golden Hour’ Concept (n=100)
C. Perception of RTI Risk Factors and Vulnerable Groups
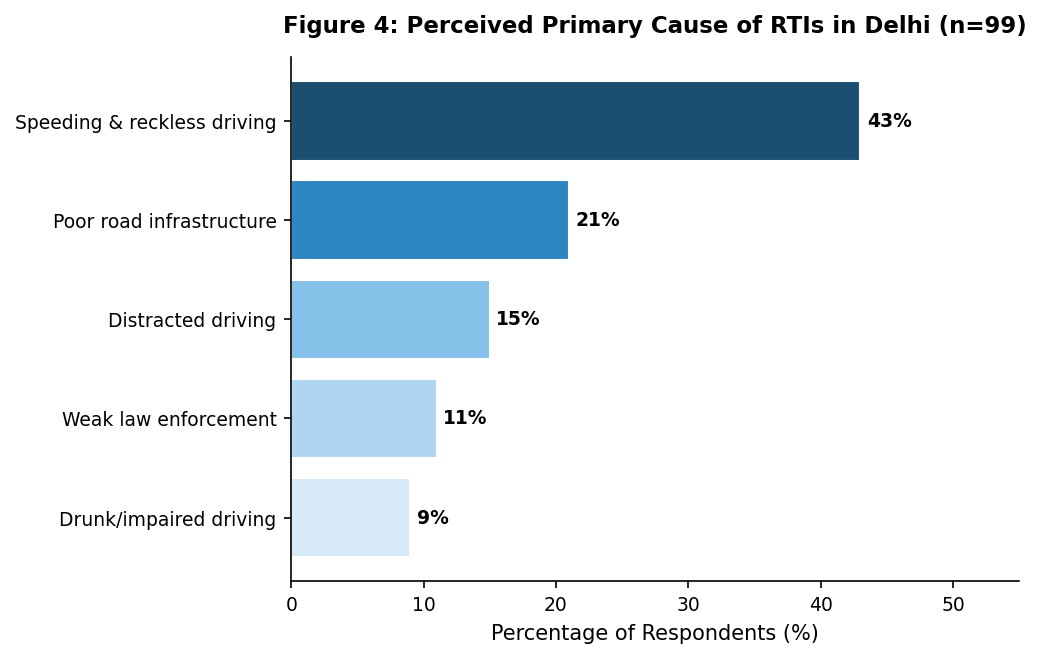
Speeding and reckless driving clearly stand out as the biggest concern, with 43% of respondents identifying it as the leading cause of road traffic injuries (RTIs) in Delhi (Figure 4). This was followed by issues related to poor road infrastructure (21%), distracted driving (15%), weak enforcement of traffic laws (11%), and drunk driving (9%).
The ranking exercise (Q13) further reinforced these perceptions. Speeding emerged as the top concern, receiving the lowest mean rank score (2.06, where 1 indicates the highest importance). Poor road design was ranked second (mean 2.43), followed by drunk driving (2.63) and distracted driving (2.78).
Interestingly, the non-use of helmets and seatbelts was consistently perceived as the least important factor (mean 3.23). This finding is noteworthy and somewhat concerning, as failure to use these safety measures is widely known to significantly increase the severity of injuries, even when other factors are responsible for causing the crash.
Figure
Figure 4: Perceived Primary Cause of RTIs in Delhi (n=99)
Normalisation bias is reflected in the under-ranking of helmet non-use: in an environment where helmet non-compliance is pervasive and observed daily, it ceases to register as deviant behaviour. This attenuation of perceived risk through habitual exposure is a well-documented phenomenon in behavioural road safety research,18 and it highlights the need for communication approaches that actively challenge and change accepted patterns of non-compliance instead of just repeating the rules.
Two-wheeler riders (65%) and pedestrians (58%) were most often seen as the road users at greatest risk of road traffic injuries, which aligns with the pattern of fatalities reported in Delhi. Respondents also identified children (42%), older adults (37%), and daily-wage informal workers (36%) as vulnerable groups. However, while these groups were clearly recognised, the deeper reasons behind their vulnerability, especially for informal workers, were not well explained in the open-ended responses. This suggests that people tend to view vulnerability in terms of specific groups, rather than understanding the broader social and structural factors that put these groups at higher risk.
D. Health Literacy and Personal Road Safety Behaviour
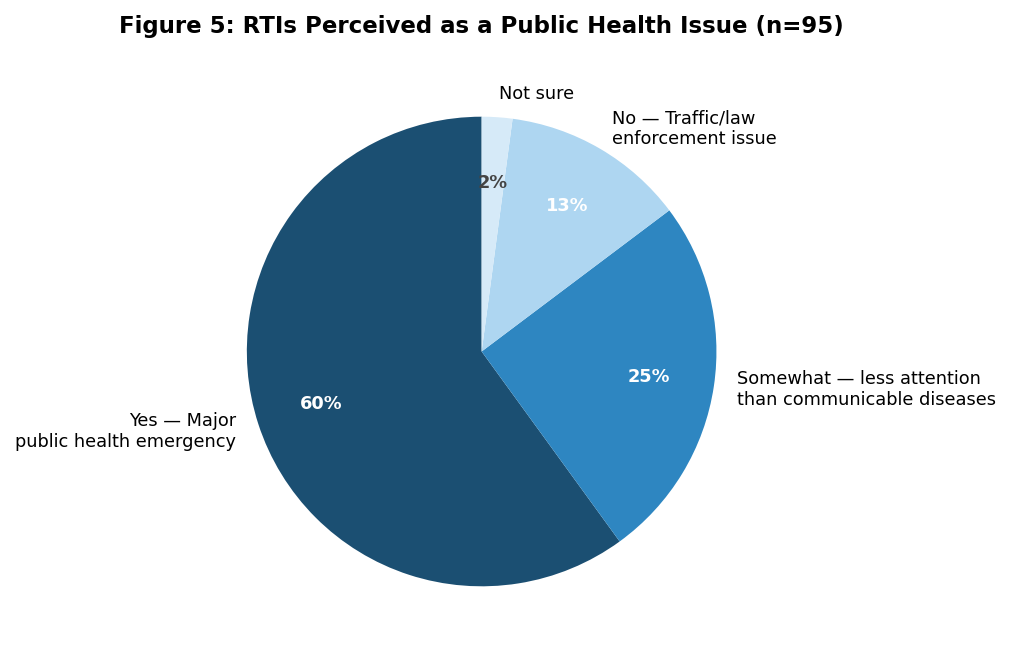
There is an interesting tension in these findings. While earlier sections revealed significant gaps in respondents’ knowledge of specific road safety laws, this section tells a different story, one where health literacy appears to outpace policy literacy. The majority of respondents (57%) recognised RTIs as deserving the same public health attention as communicable diseases such as tuberculosis or diabetes (Figure 5). Another 24% acknowledged this to a degree, though with the caveat that road safety typically receives less institutional priority. The 12% who viewed RTIs solely through a law enforcement lens were, reassuringly, in the minority.
Figure
Figure 5: RTIs Perceived as a Public Health Emergency (n=95)
This public health framing is a significant conceptual basis for health-literacy-based intervention: individuals who perceive RTIs as a health concern rather than merely a regulatory issue are more amenable to communication strategies focused on health consequences. Fifty-three percent said they fully understood the long-term effects of RTIs, such as disability, post-traumatic stress disorder (PTSD), and financial burden. However, 38% said they understood the physical effects but far fewer (6%) said they understood the psychological effects, and 6% said they did not understand them at all.
The Likert-scale health literacy statements (Q18) confirmed this trend: 87% agreed or strongly agreed that RTIs result in long-term physical disability, and 82% agreed that the mental health ramifications for accident survivors are significantly overlooked, a notable statistic that exists in productive tension with the 38% who admitted to a limited comprehension of those ramifications. Respondents acknowledge the oversight of psychological repercussions, despite lacking comprehensive understanding of these effects. This indicates that focused communication regarding RTI survivorship, especially concerning mental health sequelae, could substantially enhance both awareness and motivational behaviour. Seventy-nine percent agreed that helmets and seatbelts are primarily health protection measures rather than mere legal requirements; this recontextualisation, if authentically internalised, would foster compliance behaviours that endure in the absence of enforcement.
E. Policy Effectiveness, Community Engagement, and Social Determinants
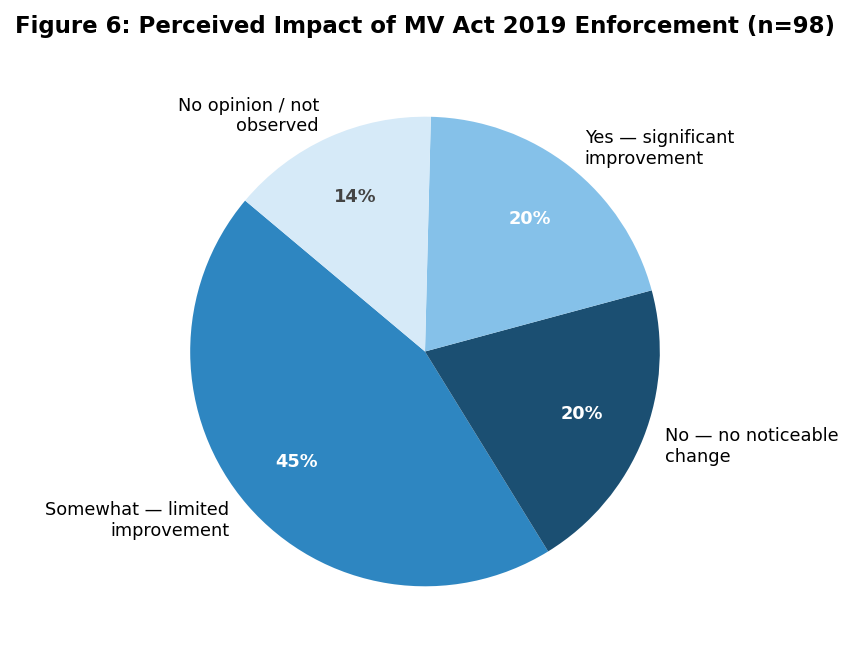
Respondents were very split on whether enforcing the MV Act had made a real difference to road safety (Figure 6). The most common answer, 44%, was that there was only some improvement in certain areas. Twenty percent of respondents reported significant improvement, while another 20% reported no noticeable change, and 14% did not express an opinion. This distribution shows a common feeling of uncertainty: most respondents said that the Act’s implementation sent some positive signals, but they did not call it transformative.
Figure
Figure 6: Perceived Impact of MV Act 2019 Enforcement on Road Safety Behaviour (n=98)
The community engagement statements in Q21 added more depth. Sixty-four percent agreed or strongly agreed that education programmes at the community level are more effective than just punishing people who break the law. This is a strong implicit endorsement of using both education and punishment instead of just punishment. Sixty-six percent agreed that socioeconomic status has a big impact on how well people know the rules of the road. This finding supports the idea that RTI prevention is about fairness, and that current communication strategies work differently for people with different levels of income and literacy.
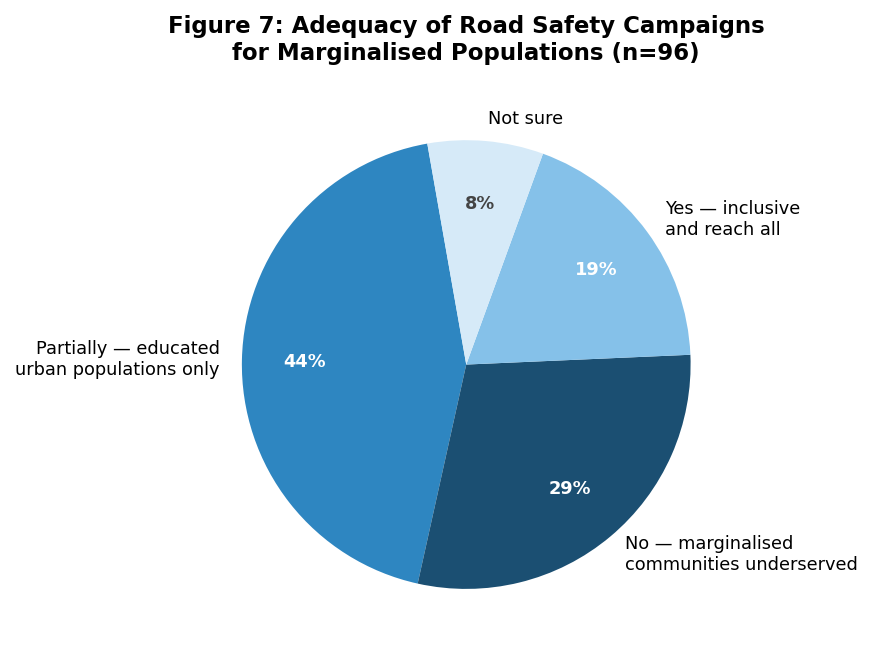
The campaign reach question (Q22) produced the study’s most structurally significant finding (Figure 7). Seventy percent of respondents, from an educated urban sample, indicated that current road safety campaigns either partially or substantially fail to reach marginalised and low-literacy populations. Only 18% thought that current campaigns were open to everyone. Since informal sector workers, people living in peripheral zones, and people with low literacy levels are the most likely to be exposed to RTIs, this communication equity gap is a structural factor that makes road safety inequality worse.
Figure
Figure 7: Adequacy of Campaign Reach for Marginalised Populations (n=96)
F. Qualitative Analysis: Critical Gaps Identified by Respondents
A thematic analysis of the 46 responses to Q25 (open-ended) and 19 additional comments yielded three primary clusters that triangulate and expand the quantitative results.
If there was one thing respondents kept coming back to, it was enforcement, or, one can say, the lack of it. Interestingly, very few blamed the law itself. The MV Act, in their view, is not the problem. The problem is that nobody consistently applies it. Several respondents described the current system as essentially reactive: traffic police show up after something goes wrong, or during periodic crackdowns, and then disappear. What people seemed to want instead was something unavoidable: automated, camera-based systems that do not take days off and cannot be negotiated with. What struck the researchers about these responses was that this was not just about punishment. Respondents seemed to understand, intuitively, that people follow rules not when penalties are severe but when getting caught feels certain. Real behavioural change, as one respondent essentially put it, only happens when you can no longer gamble on not being seen.
The second thematic cluster concerned infrastructure and safe-system design. The coexistence of high-speed motorised traffic and slow-moving two-wheelers and pedestrians on the same arterial corridors, described by one respondent as ‘heterogeneous traffic’, was identified as a structural risk factor that enforcement cannot resolve. Multiple respondents pointed out practical gaps in road design that make everyday travel riskier than it should be, such as the lack of proper footpaths, no clearly marked cycling lanes, poor street lighting, and confusing U-turns where signalised junctions would work better. These are not just minor inconveniences; they directly affect how safe people feel and how safely they can move around.
Interestingly, these concerns reflect the idea behind the Safe System approach: roads should be designed with the understanding that people will make mistakes. Instead of expecting perfect behaviour from every road user, the system itself should help prevent those mistakes from turning into serious injuries or deaths.
A third set of concerns focused on fairness, accountability, and trust in institutions. Many respondents pointed out that rules lose their meaning when they are enforced selectively or influenced by corruption; if penalties do not apply equally to everyone, people begin to question the system itself. There were also concerns about underage driving, with respondents emphasising that responsibility should not fall only on minors but also on their parents. At the same time, informal sector workers were seen as especially vulnerable, not just to road risks but also to the legal and financial consequences of accidents, which they are often least equipped to handle. Overall, these responses highlight important gaps in how current policies address issues of equity.
Policy Recommendations
Altogether, the findings of this study suggest the need for a well-coordinated, multi-layered approach rather than piecemeal solutions. Improving the situation is not just about introducing new policies in isolation; it requires a connected strategy that builds trust in enforcement, strengthens people’s understanding of health and safety, improves how infrastructure is designed, and ensures communication reaches everyone fairly. The following recommendations are derived directly from the empirical findings and are intended to be practically implementable within the legislative and institutional context of Delhi.
First, with respect to automated enforcement, the current model of discretionary, police-dependent monitoring must be progressively replaced by AI-enabled, camera-based surveillance systems operating continuously on high-risk corridors. Such a shift addresses the well-documented compliance-when-observed pattern by eliminating the uncertainty of detection altogether. Deployment should prioritise identified black spots and arterial routes with documented high RTI rates, with the goal of cultivating habitual safe behaviour rather than episodic compliance driven by visible enforcement.
Second, health literacy campaigns must be substantially broadened in both scope and framing. Road safety communication has historically centred on physical injury and mortality; however, the findings of this study indicate that the psychological consequences of RTIs, including post-traumatic stress disorder, depression, anxiety, and long-term economic burden, remain significantly under-communicated. Future campaigns should address these dimensions explicitly and target not only potential violators but also witnesses and bystanders, with specific emphasis on educating the public about Good Samaritan legal protections and Golden Hour emergency response protocols.
Third, targeted outreach for marginalised populations is essential. The study found that approximately 70% of respondents acknowledged that existing road safety campaigns inadequately reach low-literacy, informal sector, and peripheral urban communities, that is, the very groups that bear the greatest RTI burden. Dedicated, vernacular, community-based education programmes must be designed and funded for these populations, and trusted intermediaries such as local NGOs and primary healthcare workers should be engaged as dissemination channels to ensure effective and equitable reach.
Fourth, infrastructure must be redesigned according to Safe System principles, which proceed from the recognition that human error is inevitable and that roads must therefore be engineered for survivability rather than mere regulatory compliance. This entails the progressive physical separation of motorised and non-motorised traffic on major arterial roads, the introduction of pedestrian-priority crossings with adequate lighting, and the enforcement of geometric speed-calming measures on high-fatality corridors. Investment decisions should be guided by documented crash data and risk mapping rather than uniform application across the network.
Fifth, RTI survivorship must be formally integrated into the public health system. The study reveals that while respondents broadly acknowledged the neglect of psychological consequences in road safety discourse, their own understanding of these consequences remained limited. Establishing structured mental health and rehabilitation support pathways for road accident survivors would address both the clinical gap identified in the findings and the broader imperative of treating RTIs as a public health emergency requiring preventive and therapeutic responses in equal measure.
Finally, equity in enforcement must be treated as a structural policy priority. The perception of selective enforcement, whereby penalties are applied inconsistently across socioeconomic groups, was identified in qualitative responses as a significant factor undermining regulatory legitimacy and reducing compliance incentives across all road user categories. Transparent, publicly accountable enforcement mechanisms must apply uniformly, including to political office-holders and law enforcement personnel, and parental or guardian co-responsibility for violations involving minors should be formally recognised within the enforcement framework.
Conclusion
This study, based on a cross-sectional survey of 100 road users across Delhi’s five zones, shows that road safety awareness is uneven and often falls short when it comes to actually influencing everyday behaviour. In other words, while policies may exist on paper, they are not consistently reflected in how people act on the roads. Overall, the findings point to three key gaps that continue to persist and are closely connected to one another.
One of the most striking issues is a simple lack of awareness. Even after six years, nearly one in five people had never heard of the Motor Vehicles (Amendment) Act, 2019. More concerning is that some of its most life-saving provisions, such as the Good Samaritan Law and the Golden Hour cashless treatment, are still not widely known, even among educated groups. These rules are designed to encourage people nearby to step in and help during the crucial minutes after a road accident. When people do not know about them, they are far less likely to act, and that hesitation can end up costing lives.
Another important gap lies in how people understand the mental health impact of road traffic injuries. Most people are aware of the physical harm these accidents cause, but far fewer recognise what survivors often go through emotionally, conditions such as PTSD, depression, and long-term anxiety. While it is commonly said that this aspect is neglected, it is not actually well understood by the public.
In India, road safety messaging has largely focused on visible injuries and death statistics. The lived experience of survivors, the fear, stress, and psychological trauma they carry long after the accident, rarely enters the conversation. Bringing these stories and realities into public awareness could make road safety messages more relatable and impactful, encouraging safer behaviour not just out of fear of punishment, but from a deeper understanding of the human cost.
The third, and most structurally consequential, gap is that an inclusion gap exists at a significant level. About 70% of people in this relatively educated urban group admitted something important: current road safety campaigns are not really reaching those who need them the most, that is, people from marginalised backgrounds and those with low literacy levels. Ironically, these are also the groups most exposed to road traffic injuries.
This creates a double burden. The same communities that face higher risks are also the least likely to receive or understand safety information. As a result, even if overall awareness improves, these gaps persist. Without specifically designing campaigns to reach and support these vulnerable groups, road safety efforts will continue to fall short of being truly equitable.
The Motor Vehicles (Amendment) Act, 2019 gives Delhi a strong legal base to make its roads safer. But laws alone do not change reality. What is still needed is the everyday support system, a clear communication channel, inclusive planning, and safer infrastructure, that actually makes these rules work for everyone: whether someone is educated or not, whether they drive or walk, whether they travel through central Delhi or come from the city’s outer areas to earn a daily wage.
To truly make a difference, small tweaks are not enough. We need a shift in how we think about road safety, a Safe System approach. This means accepting that people will make mistakes, so roads and systems should be designed to reduce the chances of those mistakes turning deadly. It also means fair and consistent enforcement, and treating road safety awareness not as an afterthought, but as a core public health priority.
A. Limitations
The online convenience sampling method created a sample that leaned toward younger, more educated respondents. This limits the ability to generalise findings to those with lower literacy, older adults, and informal sector workers. While the sample of 100 respondents supports descriptive analysis, it restricts comparisons between different subgroups. Self-reported behaviour data can be influenced by social desirability bias, which may lead to inflated compliance rates. Future research should use stratified probability sampling, add field observation components, and expand geographic coverage to include peri-urban and lower-income areas within the National Capital Territory.
*****
Footnotes
1. World Health Organization, Global Status Report on Road Safety 2023 (WHO 2023).
2. D. Mohan, G. Tiwari & K. Bhalla, Road Safety in India: Status Report (Transportation Research & Injury Prevention Programme, Indian Institute of Technology Delhi 2009).
3. N. D. Berkman et al., Low Health Literacy and Health Outcomes: An Updated Systematic Review, 155 Annals of Internal Medicine 97 (2011).
4. K. Brijs et al., Evaluating the Effectiveness of a Road Safety Awareness Campaign with Actual Road Use as a Measure, 43 Accident Analysis & Prevention 788 (2011).
5. H. Naci, D. Chisholm & T. D. Baker, Distribution of Road Traffic Deaths by Road User Group: A Global Comparison, 15 Injury Prevention 55 (2009).
6. Mohan, Tiwari & Bhalla, supra note 2.
7. G. Tiwari, Sustainable and Safe Urban Transport in Indian Cities: Developing an Integrated Safety Management System, 24 International Journal of Urban Sciences 413 (2020).
8. R. Dandona et al., Road Traffic Injuries in Urban Areas: Need for Disaggregated City-Level Data, 26 Injury Prevention i3 (2020).
9. United Nations General Assembly, Improving Global Road Safety, G.A. Res. A/RES/74/299 (Aug. 31, 2020), proclaiming the Decade of Action for Road Safety 2021–2030.
10. World Health Organization & UN Regional Commissions, Global Plan for the Decade of Action for Road Safety 2021–2030 (WHO 2021).
11. K. P. Kaur, Governance and Public Health Synergies: Lessons from Systematic Review of Road Safety Research in India, 5 International Journal of Research in Social Science and Humanities no. 12 (2024).
12. K. Sumit et al., A Qualitative Study to Explore Traffic Police Personnel Perceptions Towards Road Safety Behaviour Among Young Riders in Manipal, India, 24 BMC Public Health 3132 (2024).
13. Akkayasamy et al., Post-Road Traffic Injury Experiences and Challenges Faced by College Students: A Qualitative Study in Madurai District, Tamil Nadu, India, 18 Asian Social Work and Policy Review e12321 (2024).
14. Brijs et al., supra note 4.
15. D. Nutbeam, The Evolving Concept of Health Literacy, 67 Social Science & Medicine 2072 (2008).
16. World Health Organization, supra note 1.
17. Nutbeam, supra note 15.
18. Brijs et al., supra note 4.